
Compiled by Greg Gibson, Physiotherapist. To book an appointment with Greg, or read his Meet the Team profile CLICK HERE.
New to running? Returning to running? Experienced and pushing yourself?
Auckland's lockdowns has resulted in gym closures and a surge of people hitting the parks and pavements running. Either to try and keep fit, for general health benefits, training for potential races or to blow off some steam.
These runners are increasing their distance run (volume) and the pace (intensity) at which these runs are done at - either from an existing level, or sometimes from nothing at all.
These increases can in turn lead to an increase in calf strains. These strains, which can be surprisingly innocuous, can be like lockdown itself, slow to resolve and then repetitive in nature. After the first lockdown period there was noticeable increase in people presenting with calf problems with a relatively similar presentation. For this reason, we at Auckland Physiotherapy, thought it may be worthwhile exploring this topic to educate you regarding this issue and some simple tips to try and avoid this injury or recover from it.
Anatomy:
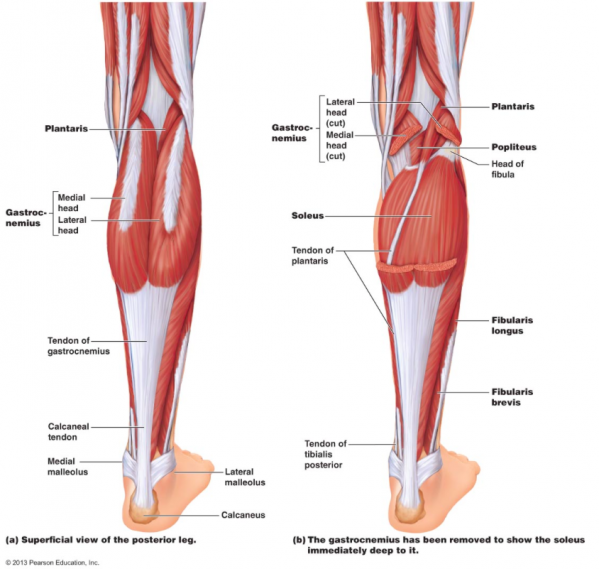
The calf complex is made up of two main muscles, your gastrocnemius and soleus, and your plantaris to a lesser extent. All three muscles join to form your Achilles tendon, which inserts into your heel bone.
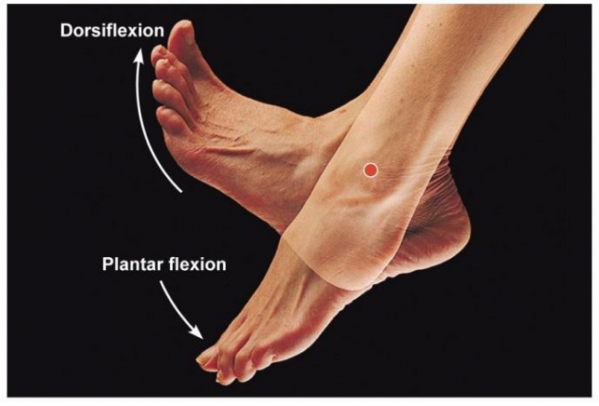
The gastrocnemius is the more superficial muscle which travels over your knee and ankle joints (bi-articular) and is therefore more susceptible to injury. Its main function is to plantar flex your ankle joint when your knee is straight and bend your knee, to a lesser extent. Generally with injuries to this muscle it is to the medial head (inside of the calf), occurs when the knee is straight and ankle is dorsi-flexed and occurs early on in activity. It occurs mainly in sports involving explosive or change of direction movements but can also occur in slower steady state running.
The Soleus muscle is deeper than the gastrocnemius and travels over the ankle joint only. It acts to plantar flex the ankle joint predominantly when the knee is bent. It also acts as a huge postural stabilizer.
Injury Presentation:
For runners there are two main presentations of calf injuries.
Acute/Sudden onset:
You’re out enjoying a run and all of a sudden you feel like someone has kicked you in to the back of the lower leg, usually located towards the inside of the calf. This is usually accompanied with a sudden sharp pain with/without a “pop” or tearing sensation. It can be painful to touch with associated swelling and bruising a couple of hours after the incident depending on the severity of the injury. You may or may not be able to walk immediately after the incident. This mechanism is usually associated with the gastrocnemius muscle and occurs when the knee is close to extension with a dorsiflexed ankle.
Gradual onset:
Injuries to the Soleus are usually more gradual in nature. Pain or a gradual feeling of tightness that gets worse may appear during a run and the pain gets worse the more you run to the point where you have to walk. It is usually injured when the knee is bent and is similar in location tp a Gastrocnemius strain where it is felton the inside of the calf. Soleus injuries are less dramatic in presentation but often have a higher re-injury rate.
Management:
Managing pain and swelling in the first 4 hours after injury is beneficial.
Rest: Avoid being on your feet too much in the early stages after injury and make sure to avoid activities that increase your pain. If needed, depending on the severity of the injury, the use of crutches can be beneficial to promote recovery.
Ice: Ice can be useful in the first 48 hours for pain control. Application to the painful site for 20 mins hourly can help control pain. Make sure you have something between your skin and the ice pack (cloth or towel) to avoid an ice burn.
Compression: The use of a compression bandage early on can limit swelling and therefore help in the healing process. The use of a compression bandage throughout the day can be useful but make sure to remove at night.
Elevation: Many people are familiar with elevation but it is no good unless you elevate the injured site above the level of your heart to allow gravity do its job and promote the mobilisation of an swelling in the area.
After the initial 48 hours it is encouraged to start to strengthen and rehabilitate your calf. This is in order to promote early healing and to prevent any muscle wasting to occur.
Prevention:
Mobility - Having a calf complex with full mobility is a good start. In general the calf complex is designed to be slightly tight in order to produce force but making sure range of motion is within normal limits is important. Due to different calf muscles it is important that you stretch them with both a knee straight and a knee slightly bent to target both gastrocnemius and soleus. Foam rolling and/or trigger point release can also be done to help with this.
Strengthening - When running at a steady state, your calf muscles are working at near full capacity, therefore having adequate strength in these muscle groups are essential. Runners need a higher level of endurance in these muscles and like mobility, targeting these muscles with a straight leg and a knee bent to above 60 degrees is recommended to target both muscle groups.
Load management - Being mindful of managing the distance you are running per week and the intensity at which you do this. Frequently people will increase the distance they run without taking into account the body's ability to respond and recover.
A personalised assessment and diagnosis from an expert Physiotherapist is always essential in order to properly diagnose and identify factors possibly leading to your injury - and then to plan out your individual recovery plan.
To book an appointment please contact reception on 09 3664480 or [email protected]




Recent Comments